

Our first challenge with this piece was to raise awareness of the Millennium Development Goals (MDGs) — a set of eight targets set out by the United Nations in 2000 to reduce poverty, hunger, and disease around the world. We were particularly focused on MDG4, which aims to "reduce by two-thirds, between 1990 and 2015, the under-five mortality rate."
Even with the considerable progress made in the last decade, we will likely fall short of achieving this goal.

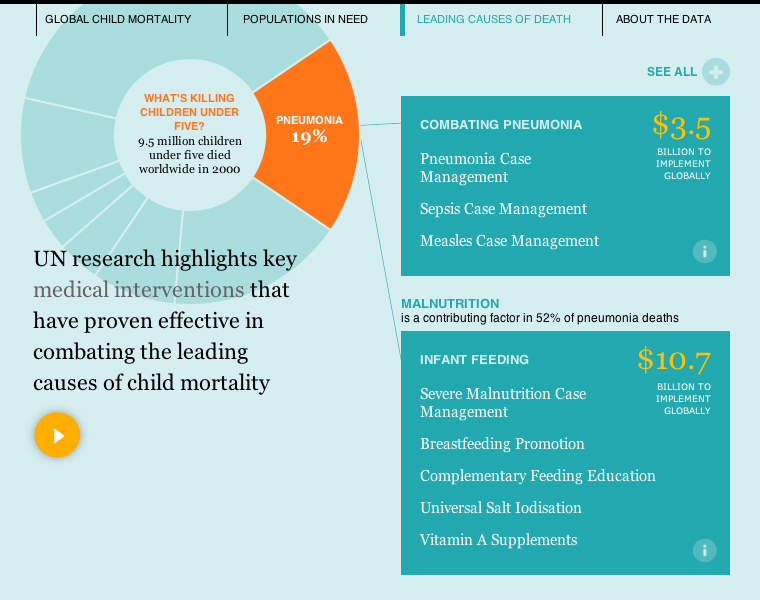
The sad reality is that the leading causes of child mortality around the world are still preventable conditions: pneumonia, diarrhea, malaria, and malnutrition.
The MDGs were (and still are) ambitious and far-reaching goals, and their publication released a flurry of funding for research to help nations achieve them.
The Lives Saved Tool, or LiST, was a key tool to rise out of MDG research. Epidemiologists at Johns Hopkins aggregated research on the effectiveness of dozens of different health interventions, and then layered that information on top of existing data for population, health coverage, birth and mortality rates. What resulted was a powerful tool that policymakers could use to model different scenarios as they planned for 2015 — an epidemiological Sim City, without the interface, and far more serious.
Out of LiST came a shorter list of health interventions that were widely recognized as efficient and cost-effective against the leading causes of child mortality. A different team of researchers then went about figuring out what it would cost to make sure all children had access to them.
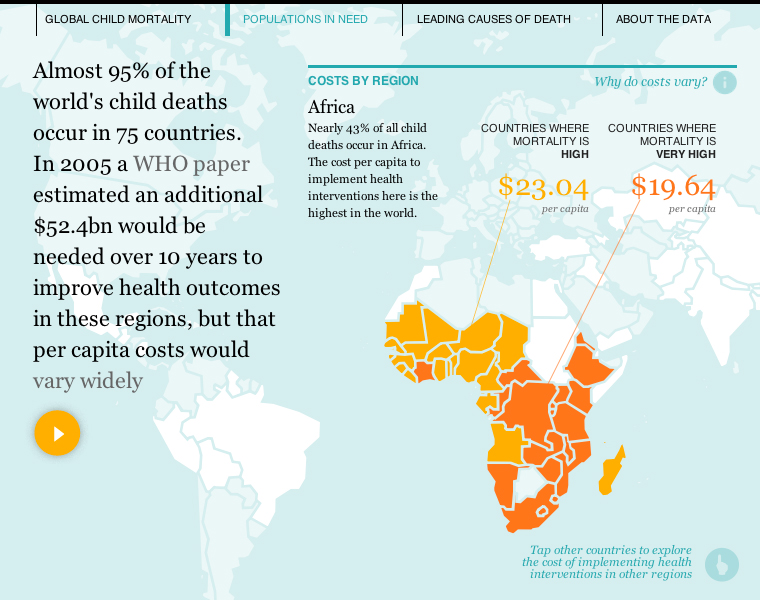
Calculating this cost is a more complicated problem than it seems, particularly when you begin to look from region to region. Some areas, such as Africa, struggle with disproportionately high mortality rates and relatively weak health infrastructures — the sheer volume of people that need to be reached means high costs for building infrastructure and buying supplies. For regions with strong health infrastructure and low mortality rates, the challenge becomes that of the long tail — with relatively high market costs for labor and drugs.
The second challenge for the Fathom team was in aggregating data from so many disparate sources. Population modeling is already a multivariate problem, and when combined with shifting political, economic, and academic climates, finding common threads across different research papers proved challenging. We culled a set of a dozen papers from the UN and WHO down to a set of four that were published over a span of 10 years, then combined that information with LiST to produce the final result (a detailed list of each source is included in the About the Data section of the interactive).
There are many different research groups focusing on the MDGs, from many parts of the world, but their findings aren't necessarily intended to be combined into larger narratives (without considerable caution). In conversations with domain experts, however, it was clear that the benefits of showing the bigger picture of child mortality far outweighed the limitations of the data.
View the original piece in the Guardian, or the writeup from the Gates Foundation's Impatient Optimists blog.
We’d love to hear what you’re working on, what you’re curious about, and what messy data problems we can help you solve. Drop us a line at hello@fathom.info, or you can subscribe to our newsletter for updates.